The Annual Subscription is being kept at the incredibly low price of just $35. I sell no bullshit supplements, no crappy merchandise, no whacko gadgets, I have no sponsors, no advertising and everything is possible to read for free. However to help in running the experiments and to cover the huge costs that are mounting from travel and expenses to operate the project, please consider donating to the largest Crowdsourced and Opensourced experiments falsifying Virology. Thank you.
The Virology Controls Studies Project is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
I am doing what I am doing with the Virology Control Studies Project for one reason: So that my children and my children’s children never have to go through 2020 again, be ostracized from society, banned from access to all social and leisure facilities because of a decision to make entry to society predicated on injecting a toxic substance into their and my veins. So when it comes to this topic, I would think and hope, like most parents, I hold my children’s health in the highest of priorities. For even the social credit and freedom to walk around this planet unrestricted still actually plays second fiddle to being healthy whilst doing it. So the decision to not get myself or children stabbed with a syringe full of shit was an easy one, but one that should never have come with conditions of relinquishing that liberty.
As part of this project I have given my reasons for my worldview on No Virus, No DNA and No Contagion of Biological Pathogens and backed them up with not only volumes of theoretical evidence but in the case of Viral Existence with rigorous experimental evidence. These areas of research have a Bi-directional benefit in that hopefully they operate simultaneously to protect you against not only tyrannical political machinations by providing solid rebuttal to political health claims such as Lockdowns and Mask Mandates, but maybe more importantly to protect you against the toxic Drugs and Medical Interventions predicated on the first.
If you truly understand the full, 360 picture of what No Virus, No DNA , No Contagion of Biological Pathogens means, the ramifications of these things rules out a large chunk of the allopathic medicine model and medical interventions. All of the Vaccines, Drugs and medical procedures become surplus to requirements when dealing with non existent causes and erroneous causes in the case of Bacteria, Parasites and Genetics. The last of those, once again, if you truly understand the Genetics hoax, casts aside many many avenues of poison drugs and death and disease causing pathways to prevent and combat an invented cause for ill health.
I am well aware that this may be a bit too much of a broad brushstroke to deal with; for the topic of health is really quite large and also, I would very much hope that you are skeptical of any intersection between the fraudulent worlds of Science and Medicine. I guess this is really the crux of the matter in that I shouldn’t really expect you to transfer any thinking between these wildly independent and separate institutionally fraudulent subjects. If I demonstrate one to be wholesale bollocks as I have started to do with Science, then that may not necessarily mean that the Medicine and Health part are too. I know they are, but that doesn’t really help you now does it?
For I have always been frustrated with the lack of logic, particularly surrounding alternative drugs and supplements, whereby in my mind, if there is a fault in the logic in scientific terms at any of these causal intersections, then that must rule out its medical usage. Once again, to me that is the case, but then I have not put into the public sphere everything that is in my head (I have a backlog of articles waiting to be written for the rest of 2026 FML), hence it is not strictly a given that you should also rule these things out.
So I am going to add to the roster of my writing the specifics on any of these areas of health/medicine/supplements/alternative cures and what I believe to be helpful. I am not going in off the deep end and full blown health guru by any stretch of the imagination, for the simple reason that I recommend basically doing nothing: Your body is brilliant, help it to heal itself, there that’s it, my health guru course in a nutshell…. Pay me. lol. But what I am going to do is flesh out the full take down of these things, much alike I did in my article “Chemotherapy is Mustard Gas”.
Ironically as well, I am not, in this article going to be too specific about a drug or new protocol or intervention, this is very much a general viewpoint as you will quickly come to tell, but it is a viewpoint that changed my life forever and one that made me view lots and lots of things simultaneously through a polar opposite lens. Hence I believe this to be the single most important piece of information on the topic of health:
CLICKBAIT
I was going to write this at the top as some sort of disclaimer, because I realize that the title is fucking inflammatory, if you have read this far and not blurted out in the comments yet about how offended you are that I would even dare to ask such a question then I have probably explained myself well already. But just to clarify, that is not a question I’d ever ask, as I know the answer, of course.
About 70% of the reason for the title is purely because actually writing the title from from the perspective of this article would have been extremely long and tedious. The remaining 30% is, I admit, for the shock factor, as I think to express the sheer gravity of the implications of the topic of this article one has to have the face-melting reaction of intersecting horror, confusion and disgust that comes with it:
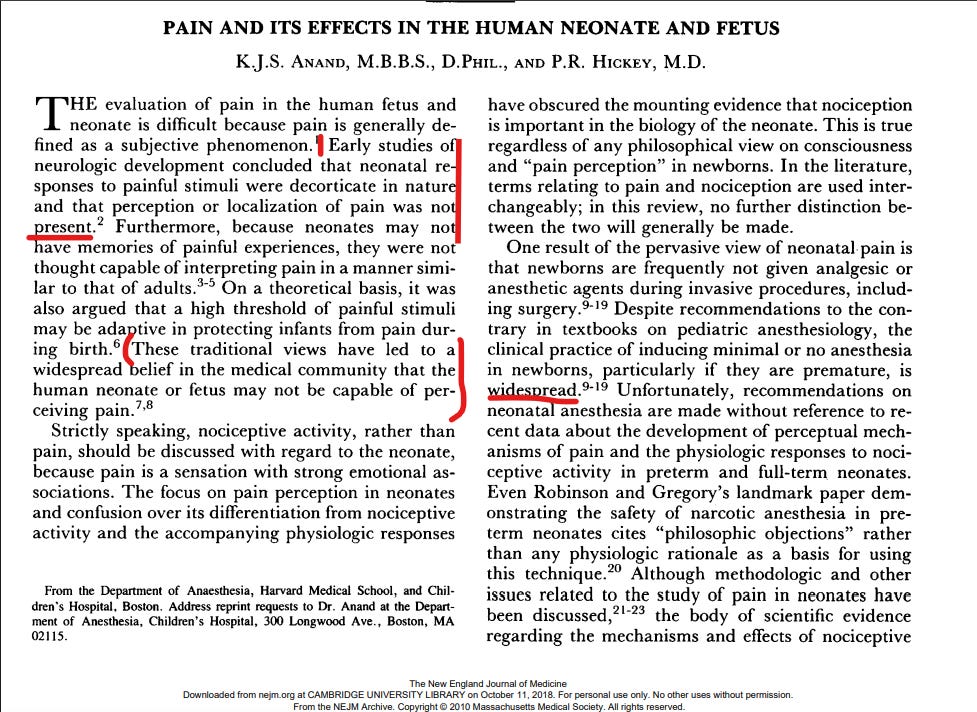
UNTIL 1986 (1999 for Premature babies) THE ENTIRE WESTERN MEDICAL ESTABLISHMENT THOUGHT THAT BABIES UNDER THE AGE OF 1YRS OLD COULD NOT FEEL PAIN AND THEIR CRIES WERE INVOLUNTARY NERVOUS SYSTEM RESPONSES.
I am going to stop there and let that piece of information sink in for a while before the next stage:
AND THEY USED TO PERFORM SOME SURGERIES, SUCH AS OPEN HEART SURGERY WITHOUT ANAESTHESIA .
I apologize profusely for the upsetting image, it is one that has stayed with me ever since I first saw it on Twitter, but this is the reality of the Medical Establishment and if you want a true and honest and well researched opinion on how they go about their business then we have to be able to see their “work” for what it is, in its complete and grotesque form. Only when we learn these hard truths can we change ,first as individuals and then hopefully as a society.
Now, as mentioned, I very first saw this as a meme on Twitter, and even the most casual surfer of the Social Media sewer should know that, when you see stuff like this, it is usually, total and utter clickbait bullshit. Especially given that the claim is absolutely wild and it is combined with an offensively sad image. Usually these things contain very small nuggets of truth that are blown completely out of proportion, so much so that they really devalue the notion. I should by all tokens have disregarded it as complete rubbish but the person that shared it, happened to be a friend of mine. So I checked and…… unfortunately it was true:
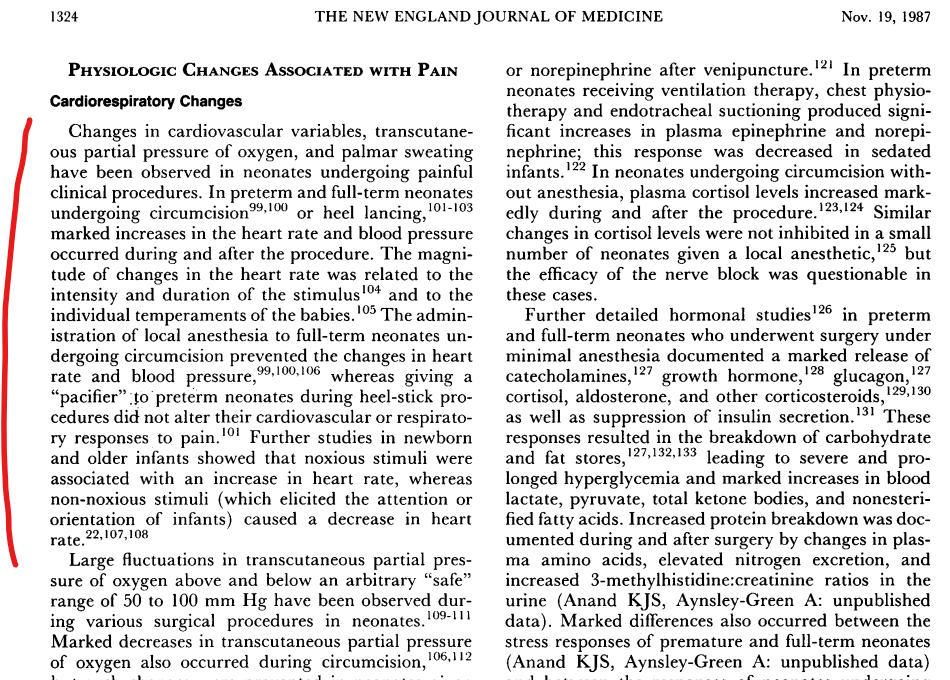
This popular precept was challenged by accumulating data on hormonal-metabolic responses to surgical procedures performed under minimal anesthesia9,10, which were effectively reduced by giving potent anesthesia11-13, the identification of a “pain system” and initial data on its early development, rich observations on crying activity and other behaviors of newborns subjected to painful stimuli in the NICU – all of which contributed to a scientific rationale for neonatal pain perception and its clinical implications3. Once the existence of neonatal pain was acknowledged and methods for clinical assessment had been validated14,15, the stage was set for advances in neonatal pain management.
Numerous clinical studies have demonstrated that failure to treat pain leads to short-term complications and long-term physiological, behavioral, cognitive sequelae including altered pain processing, attention deficit disorder, impaired visual-perceptual ability or visual-motor integration17-19, and poor executive functions20,21. Conversely, other studies showed needless analgesic therapy prolongs need for mechanical ventilation, delays feeding, or leads to other sequelae including impaired brain growth, poor socialization skills, and impaired performance in short-term memory tasks17,18. About 460,000 neonates in the US require care in Neonatal ICUs (NICUs) each year and are exposed to acute pain from invasive procedures or prolonged pain from surgery or inflammation22-24. Assessing neonatal pain is difficult to teach, time- and labor-intensive, often open to subjective interpretation, and a source of conflict in NICU care.
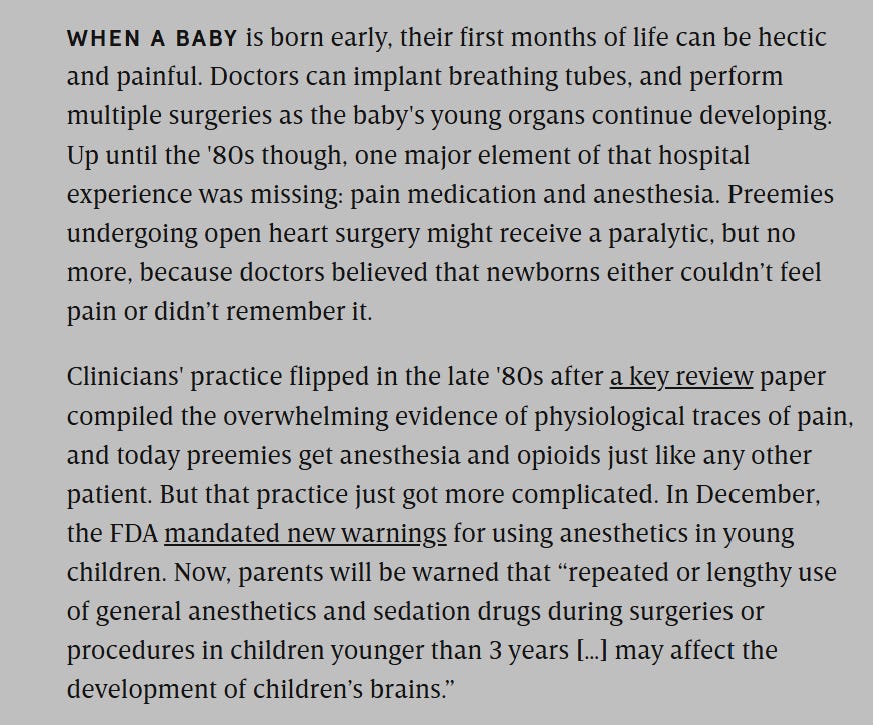
Until 10 years ago, pain and discomfort in the newborn were not seen as a priority. Babies were operated on with little or no anaesthesia and no analgesia. Babies receiving intensive care were rarely sedated. Attitudes and practices changed quickly following the publication of two key articles, so that pain and its relief are now seen to be important. The major factors in this change were the realization that the newborn feels pain, and demonstration that anaesthesia and analgesia appear to be safe. Ethical issues are raised by the fact that clinicians ignored the existence of pain in the newborn for so long.
Introduction
Over the past 20 years, advances in patient monitoring and anesthetic techniques coupled with a better understanding of the pathophysiology underlying neonatal disease states have made a great impact on the practice of neonatal anesthesia. Nevertheless, whether anesthesia is necessary in neonates and what constitutes adequate anesthesia for neonates are still major concerns among parents, health care professionals, and the public. For the anesthesiologist, the issue of adequate anesthesia is paramount to providing quality medical care. Yet Lippmann et al. (1976) wrote that in surgery for patent ductus arteriosus (PDA), ‘anesthetic or analgesic agents in our experience are unnecessary,’ and in a recent article Gauntlett (1987) stated that only 85 percent of anesthetists responding to a survey believed that newborns perceived pain.
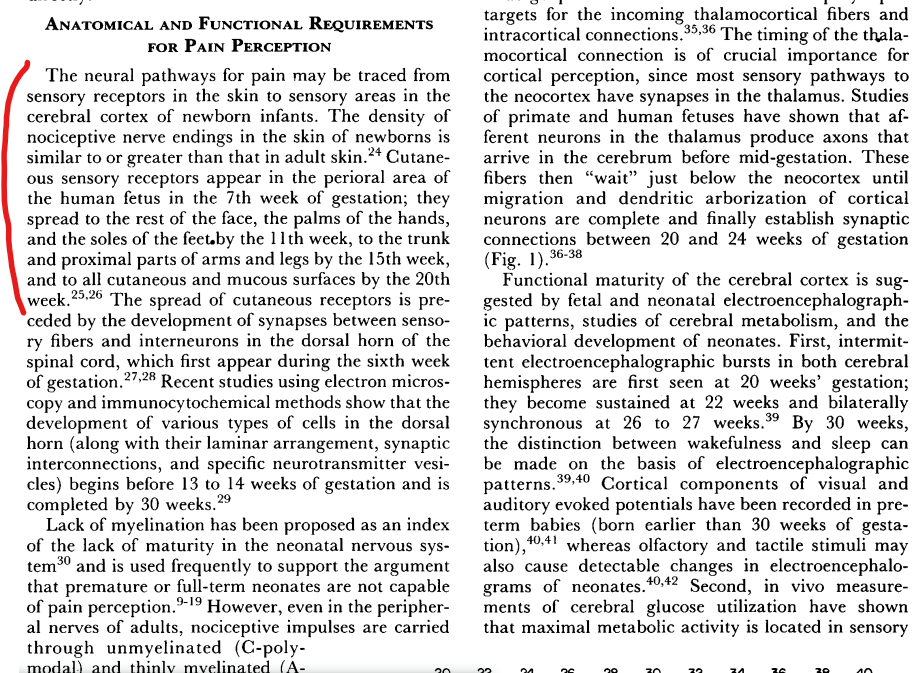
For some anesthesiologists the rationale of withholding anesthesia is still based on the notion that infants requiring surgery are too ill to withstand the significant cardiovascular and respiratory depressant effects of anesthesia. For others, the knowledge that neonatal cortical connections and nerve myelination are incomplete, coupled with the neonate’s primitive reflex (decorticate posturing) in response to pain, allow them to rationalize that operative procedures in neonates can be performed without the benefit of anesthesia.
Within the past few years, the assumption that preterm infants experience little or no pain has been challenged in nursing and medical literature. It is not clear to what extent changes have taken place in the practice area. The purpose of this qualitative study was to explore the beliefs of NICU nurses and physicians about the existence and treatment of pain in preterm infants. Respondents to the open-ended interviews were 5 neonatologists and i0 nurses at two regional referral neonatal intensive care units in North Carolina. Interviews took from 20 to 40 minutes and were analyzed using the Ethnograph program AU respondents agreed that preterm. infants experience pain. Both groups identified behavioral and physiological cues to pain recognition. There were differences in initial approaches to treatment. However, both groups indicated that the nurse has the pivotal role in recognition and initiation of treatment to reduce or eliminate pain.
CHAT GPT
🧠 What the evidence actually shows (critical clarification)
✔️ What is true
Many medical practices under-treated or ignored infant pain well into the 1980s.
Some clinicians believed infant responses were reflexes rather than conscious pain.
Major change occurred late 1980s → early 1990s, driven by:
hormonal stress studies (e.g., Anand et al., late 1980s—often cited though not retrieved above),
Fear that anesthesia was too dangerous for neonates
Belief pain might be short-lived or not consciously processed
Lack of tools and protocols
📌 Bottom line
The 1980s–early 1990s were indeed the turning point where:
strong evidence accumulated
clinical guidelines began to change
But the idea of a single “cutoff year” (1985 or 1999) is not supported by the peer-reviewed literature.
Instead, it was a gradual scientific and clinical shift.
“FIRST DO NO HARM”
At every opportunity you will invariably hear platformed Doctors and Medics spew forth this virtue signaling bilge phrase as a seemingly moral “get out of jail” free card. It broadcasts to the world around them, or anyone within earshot, that they have indeed your best interest at heart, that they haven’t got a Massive God complex, an earth shattering student loan to repay and an unquestioning belief in a medical textbook and authoritarian hierarchical structure that would make Maoist China look like Woodstock (It’s hard to find an actually truly free analogy).
For, I would say every last one of these institutionalized barbarians has been, it turns out, 100% fueled by its dogmatic religious cult like status and in unison an echo chamber of Dunning Kruger. That is my only explanation for this information above, as it cannot be passed off as a Black Swan when so uniformly presented in the faux inquisitive manner across ALL of the published literature on this subject. So let’s go through a few of the real home truths that should be ringing in your ears after reading this:
Working from the back, Chat GPT is, as one would expect, running cover for these monumentally retarded “thought leaders” of their times. It states that “not all or even most doctors believed that babies couldn’t feel pain until 1999”. This is a double edged sword for the digital version of Lord Haw Haw as really the privately held beliefs of the doctors in this cult make zero difference to how they are expected to behave in the cult. When systems and protocols are written and a chain of command is in place, you are expected to carry out the regimen written based on the beliefs of the person or people who wrote the rules ( bit of a problem, huh Statists?).
If those people, as we can see here by all of the institutional papers being put out through the 80s, 90s and into the new millennium are uniformly only at the stage of posing puzzled questions as to whether babies can feel pain or not (fucking mental) then the institution as a whole has NOT yet adopted a change. You can see this change happen from institutionally believing in BABIES FEELING PAIN (FFFFFS) in the US and Canada at least in 2006 (yes this century, yes just 20 yrs ago) when The American Academy of Pediatrics and the Canadian Pediatric Society (AAP/CPS) updated their guidelines in 2006 recommending that each health care facility treating newborns should establish a neonatal pain control program that included performing routine assessments to detect neonatal pain. Hence we can assume that institutionally beforehand they did NOT routinely detect neonatal pain because they didn’t give a shit about neonatal pain.
Really we don’t even have to be as indirect as this as in the paper “Pain in the Neonate” published in 1993, in a survey the majority (59%) of Intensive care nurses thought that babies didn’t feel pain like adults. Even in anesthetists whose sole job it is to knock people unconscious so they don’t feel pain and thrash about, 15% of them in 1987 explicitly said they believed that babies could not feel pain. This is really squared off in the first paper “Pain Management in Newborns” outlining institutional attitudes when it says “During the 20th century, however, most procedures and clinical practices established in neonatal intensive care units (NICUs) uniformly denied or disregarded the occurrence of neonatal pain”. There is no real beating about the bush as the sources lead down a reinforcing wormhole back into the 1970s the threshold where there are just no questions about neonatal pain and the protocols and hence establishment just uniformly denied it.
A CASE STUDY
It may be a little boring, so sorry for that, but I have copied this entire article in the rather tellingly named journal “Pediatric & Neonatal Pain” written by Celeste Johnston. I have included the entire article because it gives a complete picture of the thought process going on in the heads of these indoctrinated psychopathic monsters:
Abstract
From 1980 into present day, 2020, the evolution of neonatal pain research is told as a journey by one researcher, Celeste Johnston. At the beginning of her work, there was essentially no interest or work in the area. She was fortunate to be led into the area by a clinical problem: how to determine the amount of pain babies in the NICU were experiencing. That question resulted in over three decades of work with neonates. Measuring pain was the first challenge and is one that remains a focus of current research. Initially, the only choices for treating pain in neonates were either opioids or anesthetics, each with problems. Research on sweet taste and more recently on skin‐to‐skin contact has offered effective and safe options for procedural pain. Although progress has been made in the incidence of pain management in infants, it still is far less than it could be. Steps along the way of measurement, treatment, and knowledge utilization are chronicled by this researcher.
Keywords: animal models of pain, measurement of pain, neonates, non-pharmacological management of pain, pain
1. BACKGROUND
The time this story starts is early in the 1980s. When looking back, it now seems astonishing that in that era almost no attention was given to pain in neonates. There were no measures, no interventions other than opiates, which were rarely used, no policies on neonatal pain management, and prevailing myths that infants either did not feel pain or that it was short lived. I had begun working at the Montreal Children’s Hospital when finishing my doctorate in counseling psychology in 1979. For my dissertation, I studied the effect of peer models as teachers. When I first went to the Children’s, I started work on using peer models for preoperative anxiety in children aged four and older. It became clear early on, that if the pain was controlled, the anxiety was less. This is so obvious in hindsight! I had worked in an adult burn unit after my Masters degree in nursing where, being appalled at the pain burn patients suffered, I started attending pain rounds in the early days of Ron Melzack’s clinical work. I considered that I therefore knew something about pain! I started connecting with different disciplines at the Children’s in an attempt to have better management of pain in young patients, but my early focus was on verbal children.
At some point, in the mid 1980s, I was approached by nurses in the NICU to help with a problem they had regarding palliative care babies. Judi Collinge was the former Head Nurse and remained on the unit as a Research Nurse, and she and I had worked together to form a nursing research group at the Children’s1so she was my conduit into the NICU, bearing in mind that I had no clinical expertise in that population. The nurses’ dilemma was that they perceived babies in palliative care were in pain and nothing was being done for it. They wanted to know how they could prove to the medical staff that the babies were suffering. Could I help them?
2. MEASURING PAIN IN NONVERBAL PATIENTS
In searching the literature for measurements of pain in infants, there was nothing published. It was a tabula rasa. In discussions with colleagues, I did discover that in studies of facial expression or cries, pain had been one condition that had been examined. As I was working on a grant submission, unbeknownst to me, Owens and Todt were conducting research on a description of newborn pain response. Their paper was published in Pain in 1984,2and my grant was funded in 1985. The Owen and Todt study examined duration of crying and heart rate as parameters, but they had recommended more parameters be used. Happily my application had included 4 parameters including heart rate, crying duration as well as spectrograph analysis, facial expression, and body movement. We published that as a preliminary study.3
A “pain cry signature” was what I was hoping to find in the next study, along with examining developmental changes over the first year of life. My sample consisted of healthy infants 2, 4, 6, and 12 months of age coming for routine immunization. There were three conditions in which we measured their response, anger with held head so they could not turn surprise with jack‐in‐the‐box, and pain from the immunization. The pain was always last as they would have been too upset for the other conditions. There were several problems with that study. The two‐month‐olds were totally unsurprised by the jack‐in‐the‐box, and very few infants cried in all three conditions, although enough to analyze. There was a pain cry which was high pitched, long in duration, and dysphonated, which is heard as harsh.4, 5
However, I had wandered from the initial request about infants in the NICU, the ones undergoing numerous painful procedures, as opposed to healthy infants receiving an injection every two months. Two things became apparent in my multi‐dimensional approach. First of all, sick preterm neonates tend not to have the energy to cry and are often intubated, and secondly, they are (hopefully) bundled, so that you cannot see body movements. So, I decided to refocus on that population.
At the time, I was most fortunate to have Bonnie Stevens as my first PhD student. I must say that it was with her arrival that my productivity increased dramatically. Having bright, productive students is something all researchers should strive toward!
I was able to obtain funding again to study pain in infants, this time, in the NICU. Bonnie and I shared the data from the cohort of infants from 32‐ to 36‐week gestational age. In this study, we exposed infants to a sham heel lance in which heel was warmed and wiped with alcohol, and a cotton‐tipped swab is applied to the heel; then, the heel is squeezed, and motion made as though applying an adhesive dressing. The real heel lance was compared to the sham heel lance in a cross‐over design on different days. Bonnie used data from the heel lance condition for her work,6, 7, 8and I looked at the different response to conditions as well as the change over time. I was also very fortunate at that time to work with Ken Craig and Ruth Grunau in examining approaches to pain measurement.9, 10I had to confess that data were suggesting that facial expression, not cry, was a more discriminative parameter of the pain response. Ken suggested that the cry was a signal, like a siren to gain caregivers attention, and facial expression communicate what state the infant was in Ref. 11.
Bonnie and I worked with our data and developed the premature infant pain profile12which she has since tested multiple times so that it now has become a standard of pain measurement. She also tested it in older infants and for its clinical utility. It has undergone one revision to account for very young infants who may not show a response to pain.13There are a couple of unique things about the PIPP that account for the success of it. First of all, it incorporates two factors of gestational age and behavioral state at the time of the procedure, both of which impact pain response. Secondly, not widely known, the cutoff points for scoring were derived from actual data from over 100 infants, which showed a quadrimodal distribution, accounting for scoring on the PIPP of 0, 1, 2, and 3. That is, the scoring was not chosen arbitrarily, but empirically.
We noticed that some infants showed absolutely no response to a tissue‐damaging procedure, and we wondered whether there were factors that could account for that. We examine a data set from a control condition of 120 infants. We examined age, Apgar score at 5 minutes, severity of illness, sex, race, wake/sleep state, previous study sessions, total number of painful procedures since birth, and time since last painful procedure in a logistic regression. Younger age, both gestational and postnatal, sleep state, and shorter time since last procedure predicted no response.14Other studies had reported on age and state, but none had examined time since last procedure.
Although my major population was with preterm neonates, yet another bright PhD student, Manon Ranger, looked at infants in the pediatric intensive care unit (PICU) undergoing painful procedures. She used a new method, certainly new for pain in infants, to gain some glimpse of sensory cortical activity in response to pain, near‐infrared spectroscopy (NIRS).15NIRS is noninvasive and can access activity of the infant cerebral cortex through cerebral bloodflow calculations of oxygenated vs nonoxygenated hemaglobin. Thus, the amount of activity in the somatosensory cortex of the infant can be determined and has been shown to be sensitive to noxious stimuli in infants.16
3. PAIN MANAGEMENT PRACTICE
Although there were studies emerging that suggested there were important consequences to unmanaged pain (more detail below), it seemed as though there was still little being done for babies in pain, particularly for minor, but frequent procedures. Along with Judi Collinge and neonatologist, Jack Aranda, we conducted a study across Canada with 14 NICU’s to examine pain management practices.17Shockingly, less than 1% of procedures were given medication for painful procedures. This was before nonpharmacological studies had demonstrated efficacy. Twelve years later, I conducted a follow‐up survey across 14 NICU’s in Canada, not all the same as the first survey, and found that practice had improved with approximately half of all procedures being treated, all but 15% with nonpharmacological methods including sucrose which by that time had been demonstrated to be efficacious for a single procedure.18One finding that particularly interested me was that a factor predicting whether or not interventions were used was when the parent was present, their being there increasing the likelihood of management.
Another bright PhD student working with me, Margot Latimer, studied factors predicting pain management practice among NICU nurses. While expecting that multiple admissions during a shift or nurses education level and such factors to explain variation, she found that the leadership in the unit was predictive.19The more collegial and less hierarchical the nurse‐physician relationship, the higher the degree of pain management practice by the nurses.
4. CONSEQUENCES OF UNTREATED PAIN
In the late 1980s, Sunny Anand published two seminal papers that unequivocally showed that untreated pain in neonates undergoing surgery resulted in major hormonal and metabolic stress responses that contributed to increased morbidity and even mortality.20, 21These studies, along with baby Jeffrey Lawson, who died following cardiac surgery with no anesthesia or analgesia, and whose mother, Jill Lawson, published widely her baby’s completely unethical ordeal, brought the treatment of pain into the public and policy maker domain. There was newfound interest in the topic with such bodies as the American Academy of Pediatrics publishing statements about treating pain in infants.
While profound, Sunny’s studies and baby Jeffrey Lawsons needless tragic death, they did not address the daily pain that nonsurgical patients in the NICU were experiencing. Maria Fitzgerald started her pivotal series of studies demonstrating the long‐term consequences of minor procedures in infants and, perhaps more importantly, showed the developmental vulnerabilities of the preterm neonate.22, 23, 24
I decided to examine the effect of being in the NICU over 4 weeks.25I recruited two groups of infants, both 32‐week gestational age; however, one group was four days postnatal age (younger) and the other group was four weeks postnatal age. We examined the pain response and regressed factors including gestational age at birth, 5‐minute Apgars, birthweight, severity of illness, and number of painful procedures on the pain parameters of the PIPP. The older infants had a higher physiological response, that is, higher heart rate, lower oxygen saturation levels, but lower facial action expression. So, we were able to document clear changes in response over time including inability to appropriately mount a physiological response and to robustly communicate state through facial actions.
Recognizing the difficulty that I had with conducting human studies that clearly showed brain changes, this being before brain imaging studies on infants, I embarked on some animal studies with my brilliant colleague, Dominique Walker, a developmental neurobiologist. While on sabbatical in 2000, I spent time in her laboratory, her rat nursery, to learn some of the techniques used in animal models and to actually participate in the design as well as the conduction of a study to examine long‐term consequences of pain. We were particularly interested in pain sensitivity following repeated neonatal pain, mimicking experience in NICU’s. In our design, we had three groups of newborn rat pups. One group was never disturbed from the nest, and another group was simply removed from the nest and dam for 15 minutes four times daily. The third group was removed and given a pawprick with a 26 g needle and replaced in next 15 minutes later. We included the simply separated group as earlier studies had not controlled for maternal separation. We tested at ages equivalent to adolescence, adulthood, and senior age on thermal sensitivity and inflammatory pain response. There was no difference in inflammatory pain response but the separated only group had lower thresholds than the pain group, which we could not explain. When we reviewed the videotapes and counted maternal grooming behaviors when the pups were returned to the nest, we discovered that the pain group received one and a quarter times more grooming than the separated only group. When this was factored in, the pain group had a lower threshold, as has been predicted.26, 27, 28This led to an “ah‐ha” moment, which I will elaborate on later in the next section.
We followed up these studies by examining the influence of maternal grooming on pain response29, 30and continued to note that there was a blunting effect on long‐term responses with maternal influences.
5. PROCEDURAL PAIN MANAGEMENT
We were becoming aware of the hazards of using opiates with preterm neonates31and were searching for alternatives. Topical anesthetics were a group of drugs to explore, Eutectic Mixture of Local Anesthetics (EMLA) cream being one of promise.32, 33, 34We had used it ourselves in a study on circumcision.35Along with Bonnie Stevens and two neonatologists/pharmacologist, we were funded to study its use for heel lance pain management. Somewhat to our surprise, but EMLA was not effective.36A group is Sweden reported that EMLA did not have an opportunity to bind in thin infant skin.37, 38
We were also aware of the blunting of pain response with sweet taste in both animals and full terms.39, 40We then focused on sucrose. I did a few studies on sucrose, examining timing and dosage,41and comparing to other interventions such as rocking.42With Bonnie Stevens as principal investigator, we investigated the addition of sucrose to other developmentally sensitive interventions such as prone position or pacifier.43All of these studies and of others had studied sweet taste, predominantly sucrose, for a single event. Since it was showing to be highly effective, it was being used more and more in NICU’s. However, I was concerned about its continued analgesic effect as well as whether or not it would mitigate long‐term consequences of repeated pain. We conducted a study of 107 newly born infants who were less than 31 weeks gestational age who would receive 1% sucrose or placebo for every painful procedure in the first week of life. Our primary outcome was three parameters of the Neurobehavioral Assessment of Preterm Infants (NAPI), namely motor development and vigor, alertness, and orientation at 32‐, 36‐, and 40‐week gestational age. We fully expected the infants receiving sucrose to do better, but not only was there no difference between groups, when examining the sucrose group, the greater the number of doses, the lower the developmental scores.44This was the first study to indicate that sucrose was not the unequivocal answer to procedural pain.
Since sucrose was a mainstay of procedural management of pain, and some studies had found no problem with it, we decided to do a secondary analysis on the data set to see if there was a threshold of doses, below which the developmental scores were within the norms. We found that infants who received less than 10 doses of 0.1 mL 24% sucrose per week were within 2 SD of normed means of the NAPI.45
Marilyn Aita, another bright PhD student, studied the effect of environmental noise and light on pain response. She had worked in a NICU and had particular interest in Developmental Care, which is based on decreasing environmental stimuli stressors, among other practices. In her study, infants were outfitted with masks and earmuffs to blunt these extraneous stimuli, since the layout of the NICU did not allow for randomization with or without stimuli. The outcomes were indices of physiological stability, primarily heart rate variability. Unfortunately, the masks and earmuffs were distressing to the infants, so that other means of reducing light and noise need to be found.46
6. ITS ALL ABOUT THE MOTHER
Above, I mentioned the “ah‐ha” moment in our animal study when we realized that maternal grooming blunted the effects of pain. I also mentioned above that pain management was more likely to be given to an infant if the mother was there. I had anecdotally noted that babies’ oxygen saturation level increased and their heart rates decreased when a parent was beside the incubator touching them. I tried to study that by having a mat on the floor beside the incubator that had a sensor to turn on camera and capture not only behavior but heart rate and oxygen saturation level. The person stepping on the mat was to identify themselves as nurse, doctor, etc or mother, father. The machinery would also turn on for 30 seconds every 5 minutes when no one was there in order to have baseline data. Unfortunately, this study failed utterly in that nurses were straddling the mat to avoid being recorded!
I had also heard about Kangaroo Care, or more technically, skin‐to‐skin care as an alternative to incubators for preterm neonates in resource‐poor countries.47, 48Putting together my observations of the rat pups and their mothers as well as knowing of Kangaroo Care, I submitted for funding to study its effect. Just as I received word of success of funding, a study was published with full‐term infants undergoing injection that showed its efficacy.49Our first study was with infants 32‐36 weeks of age, as we thought younger infants may not have endogenous mechanisms developed enough to be invoked by Kangaroo Care. We found that it was efficacious.50We then decided to study it with younger infants, that is, 28‐32 weeks and were happy to find that it was also efficacious in this group.51At this point, we had decided to no longer have no treatment control group as there were enough data for either sucrose or kangaroo care that it was unethical to withhold.52We then conducted studies on comparing kangaroo care to enhanced kangaroo care, in which the mother rocked, talked or sang to the baby, and offered her finger for the infant to suck. There was no difference between the conditions.53In some instances, mothers were not able to be present, so we started to examine other types of kangaroo care, even just using the mothers recorded voice, which was not efficacious,54possibly because the recorded voice was too loud, which we had set to be above ambient noise, which says something about the ambient noise. We noted that at times, fathers or grandmothers would volunteer to do Kangaroo Care when the mother was not available. We then embarked on studies of fathers compared to mothers and mothers compared to other women, not related to them, since grandmothers and maternal aunts share some characteristics such as scent and voice. In both instances, the mothers were more effective than others.55, 56As mentioned above, we did not have a no treatment control group, but the pain scores from historical controls were much higher than either fathers or nonrelated women.
While conducting these studies, yet again I was fortunate to have a bright PhD student, Marsha Campbell‐Yeo who studied the effect of being cobedded with the twin in multiple births. Since these babies had been together since conception, often sharing the same amniotic sac, touching each other, we wondered whether continued care with the twin would be comforting. Using the standard of care, sucrose, as the control, we compared pain response in twins who were or were not cobedded. The pain scores were not different between the two groups of twins, but the time to recovery was less in the cobedded group57as was the cortisol response.58
Again in consideration of clinical conditions in which infants might be too young or unstable to go into Kangaroo Care, I looked for other possibilities. For very tiny infants, who are disturbed by cutaneous stimulation of any type, I decided to study Therapeutic Touch, in which direct physical touch does not happen, but rather energy fields are accessed by the therapist. The study was conducted in such a way that if we had positive results, there could be no source of bias: A site in Sweden allocated condition and only the Therapeutic Touch nurse had access to the code, and she either conducted Therapeutic Touch or stood by the incubator doing math calculations in her head with the curtains pulled around her. There were two cameras: one focused on the baby’s face for coding and one on the nurse for validation of the procedure (which were never viewed), and heart rate and oxygen saturations were obtained through clinical monitors. There were absolutely no differences between the groups.59The plots could have been superimposed. I remain skeptical about the effect of Therapeutic Touch, although people I highly respect are proponents of it.
Given our studies and the number of other studies on Kangaroo Care for pain that were coming out, we decided to do a Cochrane review on Kangaroo Care for procedural pain. We wrote one review60revised it61and are currently (year 2020) revising it to include newer studies. It is clear that it is effective as a means of preventing response from procedural pain in both behavioral and, somewhat less, physiological parameters.
We were also wanting to determine whether Kangaroo Care remained efficacious over time, whether it was as good as the standard of care, sucrose, and whether there were longer term developmental differences. We compared three randomized groups in three heel lances spread across the entire NICU stay: 24% sucrose alone, Kangaroo Care alone, or the combination of sucrose and Kangaroo Care. There were no differences in pain responses nor in developmental outcomes.62We concluded that since Kangaroo Care alone was as efficacious as the standard of care, and the addition of sucrose did not improve on any outcomes, that it should become the standard of care. We are continuing to analyze that database to examine amount of time in Kangaroo Care and even effects on epigenetics of hormones.
7. FUTURE DIRECTIONS
Being this far in my career, I am often asked to comment on future directions for research on pain in neonates. In actual fact, I cannot predict the future and trust that my younger colleagues will continue to work on it so as to alleviate suffering in our tiny patients. The few comments I do have are more general.
In terms of the quest to measure pain and not another state, I am not certain that such a thing is possible, because I am not certain that pain is a differentiated sensation in humans of any age, especially those with immature sensory processing mechanisms. If you consider that in the adult literature, there has been an ongoing search for some way to differentiate chronic pain from depression, but more recently, there is an acknowledgment that not only do the co‐exist, they might be the same. Similarly, for neonates, any high level stimulation, be it noise or light or pain, will cause distress which may be painful.
The effect of the mother is only recently being appreciated. We need only look at other mammals to see the profound comforting effect mothers have. Our recent studies of maternal (or other caring persons) comfort using ventral skin‐to‐skin contact is only the beginning of ways in which mothers and other caretakers can be more involved in reducing pain. The study on maternal voice that I conducted which had negative results should be repeated with appropriate sound levels. Maternal scent should be further explored. Basically, parents need to be more involved in caring for their preterm neonates. With acute observations, ideas might emerge for study.
Finally, the best knowledge is useless unless it is implemented into care. Much work is now being conducted on evidence‐based care. I applaud and encourage people engaged in that work because that is the ultimate goal of the knowledge generation.
ANALYSIS
This absolute brainlet starts out by verifying all of the aforementioned papers in that it was widespread belief that babies didn’t feel pain and that pain management was rarely given. She happened to have this wild thought about pain after working in an adult burns unit and then looking at babies crying. She made the incredible discovery that because adults could yell “My burns fucking hurt you stupid trollop go get me some morphine” and indeed babies couldn’t because they hadn’t developed the involuntary nervous reflexes to yet (Jokes), maybe it wasn’t so clear cut that those cries weren’t actually them saying “I fucking hurt you stupid trollop go get me some morphine” in baby language.
Our befuddled heroine then goes on a Don Quixote style adventure on figuring out whether indeed babies cries signify pain or not. She interestingly chose the pain from vaccination as the benchmark for something that we can all agree would make a baby cry an actual pain cry, because you’d have to be a psychopathic monster to not admit jamming an needle in the thigh of a baby would not injure them, amiright?!
Problem is that this wasn’t good enough for our heroine because some of the babies that she dealt with were tortured, I mean Intubated and their movements restricted so that her criteria for measuring pain which was their body movements were not able to be seen. So with a nice funding grant (YEY!) she teamed up with a bright young baby pain enthusiast who then conducted another study this time using the heel prick test as a bench mark for when we can all agree that intentionally puncturing the feet of a newborn should cause them to “real cry”.
Get this plot twist though “ In the late 1980s, Sunny Anand published two seminal papers that unequivocally showed that untreated pain in neonates undergoing surgery resulted in major hormonal and metabolic stress responses that contributed to increased morbidity and even mortality”. I mean who would have thunk it that that openly torturing babies and interpreting their cries as those similar to being frightened by a Jack-in-the-box would have lead to them being injured and killed!! This lead to her “Eureka!” moment when instead of looking at babies crying she turned to rats because their behavior is a more accurate representation of humans… than humans. She noticed that if you separate newborn rats from their mother they don’t like it and were better when they were with their mother (Genius stuff I know).
So her journey concludes, after 4 large grants to study the topic, that babies if they do feel pain will be better off being next to their mother whilst they are in pain and may not make as much of a fuss as if they are tied to a gurney and intubated. It was the workings of a medical genius, a heroine sent from the lord above to ease the suffering and pain that the medical establishment (she was milking for grant money) were causing to little innocent babies.
Why Are They In Pain In The First Place?
We are discussing here really just the instance that the medical establishment have decided that a baby needs some sort of medical intervention, surgery and the like and whether or not they need anesthetic or pain relief. Now I vaguely understand the call that ,given this absolute monstrosity of an establishment aren’t to be trusted, should they give morphine, sedatives or other dangerous drugs to babies as it might have detrimental effects. OK that is a good thought that maybe more drugs and more medical interventions will makes things worse, i.e more of their barbaric ways should probably limited, that sounds sensible.
But more than this, at no juncture does it dawn on these cretins that potentially these kids might not have to have these surgeries in the first place, or even they are having these things because of their allopathic death cult in the first instance. Obviously this subject could be about 10 articles in and of itself about fraudulent diagnosis in the first place, like claiming kids have cancer and things, so I can only really hint at this first step:
NHS Resolution’s Annual Report and Accounts for 2024/25, published today, highlights a record 83% of clinical claims being resolved without the need for legal proceedings.
In line with NHS Resolution’s strategy to keep patients and healthcare staff out of court, this means that 11,110 clinical compensation claims were resolved through dispute resolution processes rather than formal legal proceedings – the highest percentage ever achieved.
The report also describes how innovations such as NHS Resolution’s ‘Early Notification’ scheme for birth injury have enabled families to access compensation for immediate needs more rapidly. It also explains how NHS Resolution has worked with families and their representatives to ensure their involvement throughout the compensation process.
NHS Resolution received 14,428 new clinical negligence claims and reported incidents in 2024/25, reflecting ongoing broad stability in overall claims volume across recent years.
£3.1 billion was paid out in 2024/25 for compensation and associated costs on all of NHS Resolution’s clinical schemes, compared to £2.8 billion in 2023/24. £1.3 billion of the total clinical negligence payments in 2024/25 related to maternity.
The estimated ‘annual cost of harm’ for incidents in 2024/25 for the main clinical scheme, Clinical Negligence Scheme for Trusts (CNST), was £4.6 billion, down from £4.8 billion in 2023/24. This reduction reflects updates to discount rates and improvements in long-term inflation assumptions.
Demand for NHS Resolution’s expert Practitioner Performance Advice service continued to grow significantly, with 1,420 new and reopened requests for advice – a 24% increase on 2023/24. Requests for NHS Resolution’s Primary Care Appeals service to deliver fair and prompt resolution of appeals and disputes increased significantly, with a 31% rise in the number of cases received.
NHS Resolution’s provision for future liabilities as of 31 March 2025 was £60.3 billion, compared to £58.5 billion in 2023/24. The increase reflects another year of activity and natural growth, partially offset by changes to the Personal Injury Discount Rate (from -0.25% to +0.50%) and updates to HM Treasury discount rates.
ANALYSIS
Just so we are clear here, this sum of £3.1 Billion in damages paid out to over 11k people was for Negligence and Malpractice in the Maternity ward in one year in one country. This absolutely jaw dropping figure suggests that the real scale of damages and malpractice is astronomically higher. So lets just put into perspective that these idiots in scrubs are staring at newborns trying to figure out if their facial expressions can tell them whether they are in pain from an unnecessary surgery just performed or trapped gas. That they are also, when all is said and done being found medically negligent in 1 in 30 births. Doesn’t exactly fill you with trust, does it?
CONCLUSION
I have been accused rightly or wrongly for over generalizing large complex areas of Science. When it comes to things like the “Virus” question many people berate me for planting my feet and saying “Viruses Do No Exist”. It’s fine to me that you want to say “there is no evidence for Viruses” and respect that is however you feel most comfortable in backing your statements. I use that phraseology for exactly those functions; “backing your statements”, for as I have always remained consistent here at the Virology Control Studies Project and me as an individual, Jamie, I don’t want to be a source of authority or “expertise” that your thinking is deferred to. The truth works so much better when it is your truth and you know how best to defend and debate and market and live your truth, so ultimately it has to be what you believe in, not me. I am just here to present information that has changed my mind in the world that I experience it.
So my conclusion is an exceptionally easy one when it comes to the information laid out in the article, it is one that will be stereotypically over generalizing and tar an entire industry with a most VantaBlack colour blocking possible. One that experientially I have, so it is not just learned from this bleak look inside the minds of the people I will tar, but combining that with what I have seen and heard whenever I have had the displeasure of “admitting” myself into this institution:
There are two completely separate things that cannot possibly co-exist in this world, it is inconceivable for them to live and breathe and function in an orderly, predictable, efficient, productive way, together, sharing the same earth we tread on. That there can be both people that have attained enough God given wisdom and knowledge and experience about how the Human Body operates and what is best for its health and survival and simultaneously be people that cannot tell that the most precious vulnerable, pristine, innocent and angelic babies whether their cries are signifying pain or not.
It should not really matter the timings of how these events have unfolded and one does, even me, somehow relinquish some of the responsibility when these barbaric practices came from a time before anyone you could have direct contact with would be able to recount the horror of such a deluded scenario as someone that is meant to make you better, actually inflicts pain. Things such as Trepanning of the Skull to release evil spirits went on until the late 19th Century, so just out of touch of our generational pool. We might just look back on those types of practices as gruesome gargantuan mistakes, only to learn that effectively this practice has just been continued on to modern times under the guise of “releasing inflammation”.
The same goes with practices such as Full Frontal Lobotomy, which only saw its official end, last practiced in the 1980s (Must have been a real awakening decade). Once again was this practice really ever stopped or just diversified into chemically poisoning the brain and all of the different branches of “experimental neuroscience” masquerading as “drilling holes in peoples heads and cutting bits of their fucking brain out”.
So the medical system has little changed and really these squeamish fairytale stories of barbarism that are offered up as a comfort blanket of modern human endeavor really should be thought of as cultural wisdoms passed down to the discerning new generation, like “stay the fuck clear of the person telling you they are gonna fix you with a Black and Decker drill and a scalpel in their grip”. I see it as nothing to be ignored, when you hear of any of these historical anecdotes should you not realize they are alive and well right now, this should probably go for the State and centralized human governance in general, but for sake of brevity we’ll stick to health and medical science.
So my personal conclusion to all of this, how my mind has changed in the way that I approach the medical system is to take every single positive claim made about how anyone thinks the body works if not fundamentally apparent and subtitle it with “Yes but you also thought that babies couldn’t fell pain”. Is that unfair? No, not in the slightest. At any one second Celeste could have woken the fuck up out of her Frontal Lobe nullified, zombified, near decade long coma she found herself in and asked “Am I insane to think that we should just assume that babies feel pain, because the things we are doing to them should hurt and they look and sound like they are in pain?”
Should I tarnish people in a medical industry that have been blissfully unaware of Celeste’s moral path to enlightenment of discovering whether her former self was indeed human or not? Yes. For as we have shown many times, is that the State institutions work on protocols and chain of command and systems and legers. To be a part of a system that its core fundamental principles of pain management, like fulfilling their cult cub scout dib dob motto “First Do No Harm” must always be caveated with the raw unmitigated truth that they intentionally caused pain and suffering from the most monumentally cruel, dehumanizing and sick thought process ever conceived.
My mood change over this piece of information not only guided me into at no point submitting myself to the Allopathic Conveyor Belt of death and disease but has also shaped my view point to do with Science, especially obviously BioMedical science and therefore “Bio”Chemistry. I guess this is really where I get my accusations of over generalization from as of yet, I haven’t been particularly specific with a lot of my claims around this topic. I have done a lot more research than I have written articles and have lots to come, so more should be apparent in the future but I still feel that this topic should be caveated with this same sequitur:
If you think that you can synthesize the sun’s actions on a human body, make it into some sort of chemical, squirt it onto a pill and call it an essential vitamin, you are claiming literal God -like status, you are claiming that you can refine and harness the bringer and giver of all perceived life. That’s quite a bold claim, especially when you give those same pills to rats, they die (But that’s for another article). No even in that claim you must caveat that with the fact that these people who think they know everything about how the human body works, studying them with all of their machines and instruments, never had a single bleep bloop detector going on that said “Maybe babies aren’t just displaying involuntary nervous spasms when they cry and are actually experiencing pain?”.
I think it is fair to caveat all of these things with this disclaimer. I am not saying this should be the only point of reference to hold against them, but certainly when these topics are uninvestigated, or you hear new areas of Soyence emerging on the interwebs “Soyentists have discovered a new way to engineer the proteins in a Cane Toad’s tail that when boiled and eaten can instantly make you understand and speak Spanish” you think… ok…. that sounds marvelous, but given that you, as an entire Western Medical Establishment decided that Babies couldn’t feel pain until a couple of decades ago, I think we can pass it off as a crock.
SO where does that leave us for our positive thinking about health? It is all well and good sitting back in an armchair and calling everything “Fake And Gay”, but does this line of thinking help in anyway with our health? To that I would say, yes. For I think, and it is my opinion in health that there are two fundamentals; the understanding that your body is beautiful and if given the time a space to heal, it will do so to the best of its capabilities. But the second point that I think applies here is about discernment and truly listening to yourself and your body.
The market is flooded with nutritional advice and what you should and shouldn’t be doing to maintain your health. I can first, instantly disregard all the quacks that go down the “Sunshine Pills” route, any supplements at all for the aforementioned reasons. But ultimately I don’t know what nutrition is best, if I were to make a guess I think everyone needs a different nutrition. So it is incumbent to be able to listen to your own body, be attuned to it and recognize what seems good and what seems bad over both the short and long term. So I think that drowning out the noise of institutions telling you that you need a hole in your head and your baby is not proper crying, is a perfect way to actually switch on discernment and responsibility to learn about something so very personal as the topic of health and be able to apply that to oneself and most importantly to be applied for ones children.
Sorry for this sad topic, but I hope you have gained some insight from it.
Peace and Love.
J
If you have enjoyed this article and want to support the project with a one time donation please BuyMeACoffee, thanks!
This article is available as a downloadable EBook along with the rest of my work on ShadowBanned Library
Hospitals are luciferian temples of the occult. The medical establishment is controlled by evil and has been for at least the last 150 years. What they are doing is called trauma-based mind control and they use surgical torture and mutilation as part of this. Babies are still being operated on without any anesthetic whatsoever. These fragile, delicate souls are put on paralysis drugs (sometimes 24/7) so they cannot move or scream while the sadistic psychopaths we call doctors are torturing them. But they can FEEL everything and their bodies and their psyche will remember and it will drive their behavior, attitudes, beliefs, etc. later down the road if they survive. Circumcision (genital torture and mutilation) is a primary example of this trauma-based mind control torture - done at least 96% of the time in the US without any anesthetic whatsoever. The fact that people believed babies do not feel pain because these psychopaths told them so is an indication that Mankind has been put under a spell and is not in their right mind. Television helped with this spell and now the wireless grid, especially cell phones and cell towers, has nearly cemented this hypnosis into place. Millions of people are walking zombies glued to their scrying devices with little or no connection to reality.
You may be interested to read my books Jamie as you have stated you are committed to protecting your children. They are entitled:
In addition to my other comment, I should further state that ultrasound is causing massive numbers of premature births (and miscarriages, fetal deaths and stillbirths). Ultrasound usage is one way they are able to get so many babies into the NICU where the babies are daily and repeatedly tortured by these psychopaths. I've discussed this at length in my books listed below in my other comment.











Hospitals are luciferian temples of the occult. The medical establishment is controlled by evil and has been for at least the last 150 years. What they are doing is called trauma-based mind control and they use surgical torture and mutilation as part of this. Babies are still being operated on without any anesthetic whatsoever. These fragile, delicate souls are put on paralysis drugs (sometimes 24/7) so they cannot move or scream while the sadistic psychopaths we call doctors are torturing them. But they can FEEL everything and their bodies and their psyche will remember and it will drive their behavior, attitudes, beliefs, etc. later down the road if they survive. Circumcision (genital torture and mutilation) is a primary example of this trauma-based mind control torture - done at least 96% of the time in the US without any anesthetic whatsoever. The fact that people believed babies do not feel pain because these psychopaths told them so is an indication that Mankind has been put under a spell and is not in their right mind. Television helped with this spell and now the wireless grid, especially cell phones and cell towers, has nearly cemented this hypnosis into place. Millions of people are walking zombies glued to their scrying devices with little or no connection to reality.
You may be interested to read my books Jamie as you have stated you are committed to protecting your children. They are entitled:
Birth Trauma and the Dark Side of Modern Medicine
and
The Dark Side of Prenatal Ultrasound.
You can find them on Amazon or on my website here: https://birthofanewearth.com/2019/07/birth-trauma-and-the-dark-side-of-modern-medicine/
I've gone DEEP into exposing the evil of the medical establishment.
In addition to my other comment, I should further state that ultrasound is causing massive numbers of premature births (and miscarriages, fetal deaths and stillbirths). Ultrasound usage is one way they are able to get so many babies into the NICU where the babies are daily and repeatedly tortured by these psychopaths. I've discussed this at length in my books listed below in my other comment.