The Annual Subscription is being kept at the incredibly low price of just $35. I sell no bullshit supplements, no crappy merchandise, no whacko gadgets, I have no sponsors, no advertising and everything is possible to read for free. However to help in running the experiments and to cover the huge costs that are mounting from travel and expenses to operate the project, please consider donating to the largest Crowdsourced and Opensourced experiments falsifying Virology. Thank you.
The Virology Controls Studies Project is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
I want to say a big thank you and shout out to Virology Control Studies Project Subscriber Matt Reese for sending me some of the information on this.
The previous article on the Ebola Hoax was very sizeable, being a 71 page book on its own, so for the sake of fatigue I thought I would split this up into a second part where we really flesh out the hypothesis made in the first. From the ground up, I can be very sure that any symptoms/deaths from hemorrhagic type fever, if they are confirmed to actually exist were not caused by a “contagious virus”. We have covered this part of the hoax in plenty of detail, with mountains of theoretical and experimental evidence all back up with Peer Reviewed and Published literature. But I wanted to take this one a little further by expanding upon the hypothesis I presented that if these violently quick hemorrhagic deaths were occurring they fitted an identical symptomology and speed of onset of disease more concurrent with Arsenic poisoning as well as potentially a few other Heavy Metals such as Lead, Cadmium, Cobalt and Mercury adding to the tapestry of disease (as well as what I believe to be a specificity problem within their testing too).
Another marginal reason for doing this, is that the wave of State paid actors employed to furiously shoot flak into the air as a smokescreen, simultaneously settled on a seemingly very obvious lie that Ebola patients were being tested for Arsenic poisoning.
Q: “Are Ebola cases in DR Congo being tested for Arsenic poisoning, short answer?”
Short answer: No, not as a standard or reported practice.
Ebola cases in the Democratic Republic of the Congo are investigated and tested using established public health protocols (viral PCR testing, epidemiological tracing, and sometimes testing for other common infectious causes). There is no credible evidence or official reporting that suspected Ebola cases are being routinely tested for arsenic poisoning.
If there were a poisoning concern, it would be handled separately on a case-by-case toxicology basis, not as part of Ebola diagnostics.
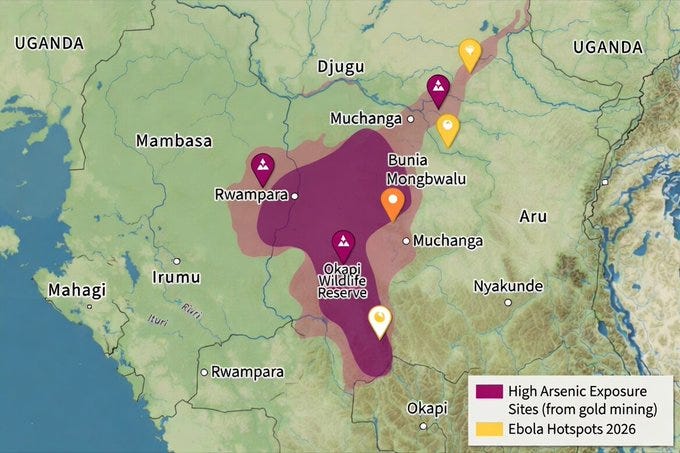
Of course this should be fairly self explanatory that once the medical authorities have been instructed that they are running the hoax simulation in their back yard, their immediate triage in a medical setting is to henceforth suspect anyone that complains of any ailment from sniffling noses to broken bones to bleeding out their eyes as being Ebola and so they are instantly going to reject any other cause for disease even if they share, or should I say especially if they share identical symptomology. Because here is the thing, Arsenic and Heavy Metal poisoning are very well known in Africa, especially in the mining communities, open cast mining releases all of these natural poisons into the air, soil and water as well as other poisons such as cyanide being used in the extraction process.
They are so acutely aware of this happening when the blinkers of infectious diseases are removed, that they have done country wide studies of Metalloid (Arsenic) and Heavy Metal poising in the environment as well as in people that both work and live in the mining areas. We are again going to focus in on one country to simplify the data and keep the amount of literature down, so we will stay in the area of DR Congo.
I’m listening to Heavy Metal
Abstract
In many countries, soil and water integrity is threatened by excessive accumulation of metal(loid) trace elements (MTEs), posing serious risks to human health. Despite increasing evidence of these impacts, contamination remains underrecognized in many regions due to limited data availability. This review compiles evidence on metal(loid) pollution across DRC, focusing on toxic elements such as arsenic (As), cadmium (Cd), cobalt (Co), copper (Cu), lead (Pb), mercury (Hg) and zinc (Zn), and their associated ecological impacts. Data were compiled from site-level studies and were analyzed using quantitative synthesis approaches to estimate pooled mean concentrations and identify regional differences. The findings indicate that Cu, Pb, and Cd occur at consistently high concentrations, frequently exceeding international reference values for agricultural soils. Spatial analyses reveal substantial heterogeneity, primarily driven by geological variability and inconsistencies in sampling methodologies. The Katanga Copperbelt provinces (Haut-Katanga and Lualaba) emerge as priority hotspots due to intensive mining activity, followed by Kinshasa, which also shows significant contamination levels.Nonetheless, a critical data gap remains in the eastern and northern mining zones, where soil quality and related agricultural risks are insufficiently characterized. These limitations, together with uneven spatial coverage and limited reporting of variance measures, restricts the robustness of comprehensive risk assessments. The review therefore underscores the urgent need for standardized monitoring frameworks, transparent data reporting, and region-specific policy interventions to enable evidence-based environmental management in mining-affected areas.
Mining activities are among the principal drivers of MTE contamination, as ore extraction, waste rock disposal, tailings storage, and acid mine drainage (AMD) mobilize toxic elements such as, Cd, Ni, Pb, Cu, Zn, and Hg, disrupting natural pedogeochemical balances (Dold, 2017; Fashola et al., 2016). Additional inputs arise from agricultural practices (e.g., fertilizers, sewage sludge, pesticides) and industrial and municipal sources, including fossil fuel combustion and inadequate waste management (Angon et al., 2024; Mohamed et al., 2025). While some metals (e.g., Co, Cu, Zn, Ni) are essential micronutrients, they become toxic at elevated concentrations, whereas Hg, Cd, As, and Pb are harmful even at trace levels (Jaishankar et al., 2014; Rai et al., 2019). These contaminants can bioaccumulate and biomagnify through food webs, posing serious ecological and human health risks (Bakshi et al., 2018; Angon et al., 2024; Sabir et al., 2022). Numerous studies conducted in agricultural, mining, and industrial landscapes have documented the widespread occurrence of soil contamination and its effects on higher trophic levels (Hou et al., 2025; Sabir et al., 2022; Haghighizadeh et al., 2024; Achouri et al., 2017). Worldwide, soil contamination affects over 20 million hectares and threatens more than one billion people via food chain exposure, with 14–17% of agricultural soils contaminated, particularly by Cd, Cu, and Co (Hou et al., 2025; Rodríguez-Eugenio et al., 2018; United Nations, 2015; Sanad et al., 2025). Consequently, sustainable remediation strategies, such as phytoremediation, are increasingly advocated to restore contaminated soils (Hou et al., 2020; Mohamed et al., 2025; Zhang et al., 2020; Reeves et al., 2017).
Fig. 5. Ecological risk indexes and classifications for toxic MTEs from mining sites.
Transfer from soils to plants and bioaccumulation of MTEs reported in RDC
For consumers, chronic ingestion of contaminated crops elevates risks of cardiovascular, neurological, renal, reproductive, and carcinogenic effects linked to Cd, Pb, and As exposure (Angon et al., 2024; Rai et al., 2019; Alengebawy et al., 2021; Jomova et al., 2025). Without interventions such as pH adjustment, organic stabilization, phytoremediation, and land-use zoning to restrict cultivation in polluted areas, both agricultural sustainability and public health remain under serious threat. In this context, integrating Land Evaluation and Site Assessment (LESA) with Geographic Information Systems (GIS) can support effective land-use zoning by identifying soils suitable, marginal, or unsuitable for food production under contamination constraints (Akbari et al., 2022), an approach particularly relevant for managing the DRC’s widespread soil contamination crisis.
Therefore, the pervasive contamination of agricultural soils in the DRC represents both an ecological and public health crisis. To mitigate these risks, integrated management strategies, combining soil pH regulation, organic amendments, controlled crop selection, and regular environmental surveillance, should be prioritized. Establishing national frameworks for soil and food monitoring would not only safeguard public health but also enhance the long-term sustainability of the country’s agricultural systems.
Abstract
Introduction
Arsenic and cadmium exposures cause significant adverse effects. This study aims to determine the urinary arsenic and cadmium concentrations in men in order to analyze their profile in relation to sperm count test values.
Methods
We conducted an exposed-non-exposed analytical study of men exposed to arsenic and cadmium in a mining area in Upper Katanga, DRC and of non-exposed men living far from any mining area.
Results
Study results show that 48% of exposed subjects had semen pH below the threshold value of 7.2 versus 16% of non-exposed subjects. The risk of a lowering of pH below the standards was more than 4 times higher (OR=4.85[1.9-12.39]) among exposed men. The difference between the averages of the total number of spermatozoa was statistically significant to the advantage of non-exposed subjects. Abnormal number of spermatozoa was much higher in exposed subjects. It was recorded a more rapid spermatozoa mobility degradation in exposed subjects. In addition, 44% of exposed men had urinary arsenic concentration > 20 µg/L versus 8% of non-exposed subjects, the risk of excessive arsenic accumulation was nine times higher in exposed men than in non-exposed men (OR=9.04 [2.82-28.96]). Sixty percent of exposed men had urinary cadmium concentration ≥0.5µg/ml versus 38% of non-exposed subjects, with an Odd Ratio of 2.45 [1.1-5.47], reflecting a risk of excessive cadmium accumulation in exposed men. On the other hand, it was recorded that, among exposed men, high urinary arsenic and cadmium concentrations resulted in a proportional degradation of sperm count test values.
Conclusion
This study shows, on one hand, high urinary arsenic and cadmium concentrations and, on the other hand, more rapid and more severe alterations of sperm count test values in men living in mining area. This suggests a decline in male fertility which deserves to be further documented in future studies.
Abstract
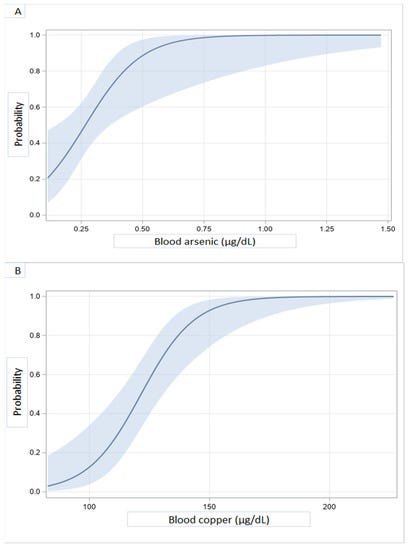
Blood and/or urine levels of 27 heavy metals were determined by ICPMS in 41 patients with dilated cardiomyopathy (DCM) and 29 presumably healthy subjects from the Katanga Copperbelt (KC), in the Democratic Republic of Congo (DRC). After adjusting for age, gender, education level, and renal function, DCM probability was almost maximal for blood concentrations above 0.75 and 150 µg/dL for arsenic and copper, respectively. Urinary concentrations above 1 for chromium, 20 for copper, 600 for zinc, 30 for selenium, 2 for cadmium, 0.2 for antimony, 0.5 for thallium, and 0.05 for uranium, all in μg/g of creatinine, were also associated with increased DCM probability. Concurrent and multiple exposures to heavy metals, well beyond permissible levels, are associated with increased probability for DCM. Study findings warrant screening for metal toxicity in case of DCM and prompt public health measures to reduce exposures in the KC, DRC.
The blood arsenic concentration found in our subjects (0.39 µg/dL) far exceeds what has been reported in the general population of France (0.17 µg/dL) [47], Brazil (0.11 µg/dL) [50], Pakistan (0.21 µg/dL) [51], and China (0.23 µg/dL) [52]. Whether the association between DCM probability and higher blood levels of arsenic implies the later may contribute to the etiology of DCM is not known, but remains a possibility. Experimental studies in rodents, however, have demonstrated the toxic effect of arsenic on myocardial tissue through the inhibition of anti-oxidative stress defense enzymes [53,54]. Arsenic exposure has been associated with cardiopathologic effects, including ischemia, arrhythmia, and heart failure [55]. Possible mechanisms include increased oxidative stress, depletion of antioxidant status, DNA fragmentation, apoptosis by mitochondrial disruption, caspase activation, MAPK signaling and p53, functional changes in ion channels, and dyshomeostasis of trace elements [55]. It has also been revealed that arsenic can induce all kinds of diseases, including heart diseases through epigenetic modifications associated with hypermethylation of genes coding for ion channels and diverse proteins of oxidative stress and energy production [56,57].
Exposure to copper is associated with increased cardiovascular risk [58]. High copper concentrations had been associated with heart failure incidence [36,59,60,61,62,63] and bad outcomes such as re-hospitalizations and deaths over a one-year follow-up [64]. Copper is an important trace element in humans that is incorporated in several enzymes of vital functions. However, at high concentrations due to permanent exposure or in Wilson’s disease, for example, its free fraction increases in such manner that its infiltrates the myocardial tissue, induces cellular toxicity, and promotes harmful free radical formation [65,66,67,68]. Although the blood concentration of copper reported in this study was slightly higher than the upper limit of the reference value (143.7 vs. 140 µg/dL) [69], the urine concentration far exceeds levels reported as reference value [44,70] and in a very high-exposure environment [38]. This high urinary concentration, which, moreover, was strongly correlated with blood concentration (r = 0.73235, p < 0.000), was precisely such an indication of a strong recent exposure. It was also an indication of a permanent exposure to this metal, which, ironically, is the great wealth of the KC. Because of copper and cobalt, the KC has been invaded by many mining companies that are the main polluters in the region.
Abstract
Exposure to heavy metals can affect cell differentiation, neurocognitive development, and growth during early life, even in low doses. Little is known about heavy metal exposure and its relationship with nutrition outcomes in non-mining rural environments. We carried out a community-based cross-sectional study to describe the distribution of four heavy metal concentrations [arsenic (As), cadmium (Cd), lead (Pb), and mercury (Hg)] in the serum of a representative population of children aged 12 to 59 months old from the rural region of Popokabaka, Democratic Republic of Congo. The four metals were measured in 412 samples using inductively coupled plasma–mass spectrometry (ICP–MS). Limits of detection (LoD) and quantification (LoQ) were set. Percentiles were reported. Statistical and geospatial bivariate analyses were performed to identify relationships with other nutrition outcomes. Arsenic was quantified in 59.7%, while Cd, Hg, and Pb were quantified in less than 10%, all without toxicities. The arsenic level was negatively associated with the zinc level, while the Hg level was positively associated with the selenium level. This common detection of As in children of Popokabaka requires attention, and urgent drinking water exploration and intervention for the profit of the Popokabaka community should be considered.
Among the various HMs, arsenic (As), cadmium (Cd), lead (Pb), and mercury (Hg) are the most common and are considered harmful9,10,11. Arsenic is widely distributed in natural waters, and groundwater is one of the primary routes of exposure to inorganic As15. Long-term exposure to inorganic As during infancy increases the risk of lower respiratory tract infection, gastrointestinal illnesses, and cancer15,16. Lead, which has no physiological role in humans, is frequently found in household dust. More than 95% of the total Pb exposure ends up in the bones and teeth. Children are particularly vulnerable to lead because of its effects on growth and the developing nervous system17. Cadmium is mainly absorbed from the lungs, and tobacco smoke is one of the largest single sources of Cd exposure in humans18. It can accumulate in fatty tissues and human milk and be transferred through breast milk to children. Cadmium toxicity negatively affects reproduction, neurodevelopment, and hepatic, hematological, and immunological systems10,18. Mercury is used in agriculture in fungicides or seed preservatives and pharmaceutical catalysts in organic syntheses. Higher levels of Hg are often found in seafood, and exposure to this element is also suspected to impair neurodevelopment in children12 and cause dental, skin, pulmonary, and nephrotic damage19.
ANALYSIS
This is a small selection of what I could quickly find on Metalloid and Heavy Metal poisoning of people in the Democratic Republic of the Congo. This not only covers people whom work directly in the mines but indeed men, women and children in the general population. Probably the most damning evidence is when these extremely worrying levels of toxic elements are found in the urine and blood of Cardiomyopathy patients. They even go as far as to suggest causality, which to you and me shouldn’t be a surprise, but it is always good to have it confirmed by the establishments own sources. When you lay it all out on a table, that these elemental poisons are known to cause the exact palette of symptoms blamed on Ebola. They are highly prevalent in the food and water sources and found in people experiencing serious Cardio and Respiratory illness, we can see that it is an entirely plausible theory to suggest that, when and where you do have real death and disease that is being attributed to “Ebola”, it is actually far more likely it is metalloid/heavy metal poisoning instead (That and because viruses don’t exist).
Please read it when you have the time as it is absolutely damning. Indeed this whole area of research is a literal gold mine of industrial harms perpetrated either directly or indirectly by the globalist operators in Africa. But the problem for me, personally with this particular article is that it doesn’t really match up with my theory in that Ghana has never had a claimed “ebola” outbreak. Now there is some wiggle room here in the fact that Ghana has seen a claimed “Marburg” outbreak in 2022 and Marburg is the identical hoax where the “Viruses” particles are identical, the symptoms are identical so we could “get away” with just continuing on oblivious. But I want to be a bit circumspect here and finish this hoax off with the final layer of the puzzle.
MONOCLONAL ANTI(Human)Bodies
Ebola-specific drugs (used once confirmed or strongly suspected in outbreak settings)
If Ebola is confirmed (or in some outbreak protocols when suspicion is very high), monoclonal antibody therapies are used:
Inmazeb (atoltivimab/maftivimab/odesivimab) → A 3-antibody cocktail targeting the Ebola virus
Ebanga (ansuvimab-zykl) → Single monoclonal antibody treatment
These are the main WHO-recommended treatments for Zaire ebolavirus disease.
Remdesivir (studied but not a standard Ebola therapy)
Other antivirals have generally not shown strong benefit compared to antibody therapies
More than 11 years ago, six young men were left writhing in agony with their organs failing after agreeing to take part in a routine drugs trial in London.
The group were part of a team of eight who were each offered £2,000 for a three-day trial that would potentially help revolutionize cancer treatment.
The men, who had been selected to be aged between 19 and 34, had been told the worst symptoms would be a headache, nausea and, in rare cases, hives.
However, soon after receiving the drug, six were left vomiting and screaming in agony – with one having to have body parts amputated.
Now, a BBC documentary has revisited the dramatic events that left the human guinea pigs fighting for their lives in a private unit at Northwick Park Hospital in north-west London run by Parexel, a US company.
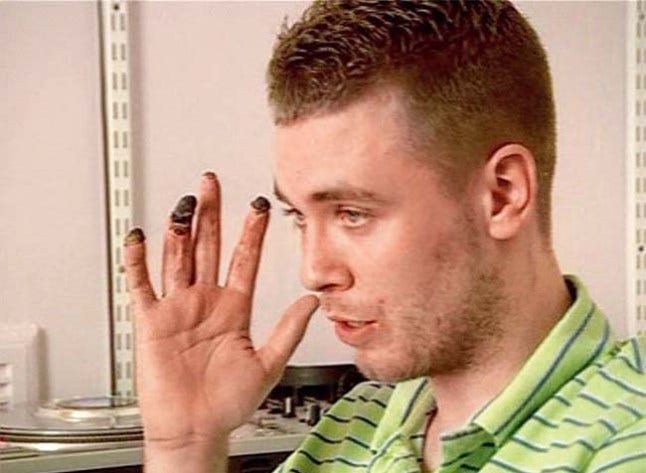
Ryan Wilson, who was 21 at the time of the trial, lost his fingertips, toes and part of his foot as a result of the severe reaction to the drug (Picture: Channel 4)
Raste Khan was unaware that he had been given a placebo but saw everyone around him screaming in agony. At 1pm on the day of the trial he was sent home and had to watch the events unfold on the news (Picture: BBC/Raw TV)
Throughout the Phase 1 trial, a number of the men suffered from swelling – with their heads inflating like balloons.
One of the victim’s family said he looked like ‘the Elephant Man’, which led to the TGN1412 legal proceedings’ nickname, ‘the Elephant Man drug trial’ – although the swelling was likely caused by the treatment for the reaction, which included administering large quantities of fluid and steroids.
The drug, which had been successfully tried out on monkeys, had never been tested on humans, making it a ‘first in man’ trial. It was later found that while macaques and humans are incredibly close from a DNA perspective, the cells that the drug targeted differ slightly between the species.
The incident quickly transformed into one of Britain’s most infamous medical emergencies.
Fortunately, doctors were able to save the lives of all of the young men – and a few weeks later, five of the men were able to leave hospital, however, the drug had attacked their tissue and left them with wasted muscles. One, David Oakley, said it had left him feeling like ‘an 80-year-old’.
Ryan Wilson, the sixth and youngest participant aged 21, spent the next four months being treated for heart, liver and kidney failure.
Sections of his feet were amputated and his fingertips also fell off.
It was later revealed that two of the participants were given a placebo and did not suffer the effects.
Participant David Oakley said he was left feeling ‘like an 80-year-old’ after the trial. His muscles were completely wasted and he feared he would be infertile (Picture: BBC/Raw TV)
All of the men had their lives saved but some suffered amputations or months of health issues (Picture: BBC)
In the documentary, The Drugs Trial, which aired last night, doctors speak about the struggles they faced while attempting to bring the ‘mysterious’ situation under control.
Investigators also reveal that they were sent in and tasked with finding out what went wrong at the trial on March 13, 2006. They found that Parexel could not have known the ‘unpredictable’ biological reaction would occur, although the risk of cytokine storm– the effect that caused the reaction – was mentioned in Parexel’s own literature with the recommendation to treat with steroids.
Participant Raste Khan, who was 23 at the time and had been given a placebo, said: ‘Medical trials were like a get-rich-quick scheme. It was a no brainer.
‘It was all manic, everything was happening all at once. They were vomiting, they were screaming in pain, people were fainting, they couldn’t control their bowels… it was like a horror movie.’
In the documentary, it was revealed that families were told to say goodbye to their loved ones as they may be about to die.
Since the disaster, all six men have received undisclosed pay-outs from Parexel in private out-of-court settlements.
A report published by The Medicines & Healthcare Products Regulatory Agency in April 2006 had 22 recommendations to improve the safety of future Phase 1 trials, including that individuals given a ‘first in man’ drug in a trial should not receive the drug at the same time on the same day and high risk trials should take place in a hospital with access to intensive care.
The new recommendations have now been adopted across the whole of Europe.
Trial lead Dr Bradford, who had worked on 300 clinical trials before this one, said he has never worked on a trial of this nature again. ‘It was the last ‘first in man’ trial I did,’ he says. ‘I’d like to look them in the eye and say sorry.’
Trial participant David Oakley was found to have pre-cancer signifiers in his blood after the trial that may or may not have pre-dated the trial.
He married his fiancee months later but feared he could be left infertile. However, 10 years on, he has three children and no sign of cancer or other lasting effects. He now says: ‘I was unlucky. But it didn’t kill me, and that’s pretty good. Having my first child with the chance that we might not have been able to have kids, made it even more special.
‘Medical trials are very important to advance our knowledge of medicine. It’s only when you have a relative who’s sick and depends on drugs that have been through human trial that you understand how important it is that they are carried out.’
In 2013, TGN1412 was tested again in human trials in Russia under the new name, TABO8. The amount was 0.1% of the amount injected into the participants of the Parexel trial and it was infused 40 times more slowly.
The drug could still be used as a treatment for autoimmune disease in the future.
Q: Inmazeb (atoltivimab/maftivimab/odesivimab) have these got any bad known side effects?
Yes — Inmazeb (atoltivimab/maftivimab/odesivimab) does have known side effects, but most are tied more to infusion reactions and the severity of Ebola illness itself rather than “toxic drug effects” in the way some chemotherapy drugs behave.
Here’s the clean breakdown.
Most common side effects
In clinical studies, the most frequently reported effects (seen in ≥20% of patients) include:
Fever (pyrexia)
Chills / shivering
Fast heart rate (tachycardia)
Fast breathing (tachypnea)
Vomiting
These often overlap with Ebola symptoms themselves, which makes interpretation tricky.
Infusion-related reactions (most clinically important risk)
Because it’s an IV monoclonal antibody, the main concern is infusion or hypersensitivity reactions, which can include:
Sudden fever or chills during infusion
Low blood pressure
Shortness of breath
Rash or itching
Dizziness or fainting
Rarely, severe or life-threatening allergic-type reactions
These are why patients are:
monitored closely during infusion
treated in high-acuity hospital settings
ANALYSIS
One of the treatments for Ebola is using that well known kidney melting drug Remdesivir, so we don’t really need to waste much time explaining the problem here. I really want to focus on the use of Monoclonal Antibodies as the “got to “ for confirmed Ebola patients. Looking at the “Elephant Men” drugs trial where they gave IV Monoclonal Antibodies that was supposed to “cure” Leukemia, i.e a blood cancer, these men in the trial very quickly started extreme bouts of vomiting, diarrhea, migraine, loss of consciousness and coma. This as they note was brought about by what they call a “Cytokine Storm” where the body floods itself with what the medical establishment believe is “immune cells” and eventually causes multiple organ failure .
The most stunning part to this story, and I really would recommend watching the BBC documentary on it if you want another example of Big Pharma and the Medical Industry’s ongoing genocide, is that this drug that almost killed the 6 men given it, was released back onto the market! They changed the made up acronym from TGN1412 to TAB08 and then used it at 0.1% concentration. Jaw-dropping really, but when you realize that the entire allopathic death cult is predicated on giving people little bits of poison until they either get better on their own despite the poison for the disease to come again soon or die from the poison.
Finally when we looked at the specific Monoclonal Antibodies used for Ebola, funnily enough they outright admit that the known side effects exactly match Ebola symptoms which makes “interpretation tricky”. Well yes indeed it would make it tricky if the drug you were giving people were causing the symptoms you are giving the drug for, that’s kind of where we are on this House-of-Horrors-Roundabout-Groundhog-Day-Purgatory we find ourselves burdened with when it comes to navigating the “health”care industries.
“EBOLA” Patient Dr. Ian Crozier
I want to leave you with the story from the mouth of a claimed “Ebola” survivor, Dr . Ian Crozier. Because this is going to be put into Ebook format that doesn’t have video embedded into it, I would urge you watch the full video here.
There are a couple of absolute zingers I want to point out to you from this testimony. Ian has very basic low grade symptoms of a fever, muscle aches and a headache, which could be interpreted as basically any disease in the entire smorgasbord of relabeling detoxing. The “emergency” situation was not brought about by symptoms at all, but would you know it was entirely started by a Positive PCR test (huge eye roll). Ian recounts this next phase in quite a bit of detail (because it is the last thing he remembers) that he was, in his own words, “clearheaded” and “fairly well”. However the moment he crossed the drawbridge into the Medical Dungeon was the moment it all seemed to go pear shaped (color me shocked I tell you). He developed severe gastrointestinal symptoms, vomiting and diarrhea, then a Cytokine Storm bringing about multiple organ failure.
Now, I mean called me cynical, but this man in his own words was “fairly well” and then displayed the identical symptoms of what can only be described as Monoclonal Antibody poisoning directly mirroring the poisoning of the “Elephant Men”. I hope you can see very clearly what is occurring here, well people with generic symptoms are being systematically maimed and killed with proven lethal chemical cocktails based on a PCR test and politics.
If you have enjoyed this article and want to support the project with a one time donation please BuyMeACoffee, thanks!
This article is available as a downloadable EBook along with the rest of my work on ShadowBanned Library
"I'm listening to heavy metal". Good one, but I don't believe it.
The level of toxicities these subsistence-scratching people are exposed to is astounding in it's breakdown, after reading just these two papers you quote here re the Congo. And not only the miners (including children), but everyone else "downstream", literally.
Toxicity is very real, with even mainstream acknowledgement, but Rockefeller medicine never lets poisoning get in the way of a good virus story. Here's one story re arsenic sent to me by JAMA (I let them send me their free stuff): https://jamanetwork.com/journals/jama/fullarticle/2841553 .....study in Bangladesh, referencing well water .... "Question: Is reduced arsenic exposure associated with reduced chronic disease mortality?"
"Findings: In this 20-year prospective cohort study of 11 746 adults in Bangladesh, participants with greater reductions in urinary arsenic had significantly lower mortality from chronic diseases, including cancer and cardiovascular disease, compared with those with persistently high exposure."
And after reading about monoclonal antibodies and "elephant man", coupled to my own research, it's one again emphasized, as you put it, big medicine is "predicated on giving people little bits of poison until they either get better on their own despite the poison,... or die from the poison."
Thanks for the Ghana/marburg reference. It brings up another little point; use of language, specifically that used to sensationalize, propagandize, or cause fear. There are plenty of search results for the marburg/Ghana story, so I just went with Wiki:
"In July 2022, an outbreak of Marburg virus disease occurred in Ghana.[1] Two positive cases were reported by Ghana on 8 July. After confirmation by the World Health Organization, it is the first such outbreak in Ghana. Two men aged 26 and 51 years old were infected with the disease and both cases resulted in fatalities. An additional case was identified, bringing the total to three.[2]"
Just to summarize, we have here 3 claimed cases, and this is called an OUTBREAK. If there happens to be 3 claimed cases of "flu" here in the state of Oregon, are we suffering an outbreak?
So Wiki sums up: "The outbreak was confirmed by the World Health Organization on 17 July 2022, making it the first such outbreak in Ghana.[11] The outbreak follows another that occurred in Guinea the previous year.[12]"
So, moving on to the Guinea OUTBREAK, I'm told:
"The index case, a 46-year-old farmer from Temessadou M'Boké village in Guéckédou prefecture, got his first symptoms on July 25.[6] The patient died on August 2. On August 3, a Polymerase Chain Reaction (PCR) test was conducted, returning a positive result for the Marburg virus on August 5. The WHO was informed of the first case the next day. On August 9, the Institut Pasteur Dakar in Senegal provided reconfirmation that the result was positive for the Marburg virus.[6] Sequencing of an isolate from the Guinean patient showed that this outbreak was caused by the Angola-like Marburg virus.[6]
"Guinea health authorities conducted contact tracing and monitored 170 known high-risk contacts of the index case. No new cases were detected for twice the length of the incubation period of the virus, in this case 42 day, so the outbreak was declared over around six weeks after it started.[2][1]
"WHO's Africa director Matshidiso Moeti, among others, praised Guinea's rapid and effective response to the outbreak.[7]"
What fun. Here we have an "index case" of ONE (that's number 1), leading to, or should I say "being" an outbreak. An outbreak of 1....
More fun stuff is described, including WHO specialists showing up to trap bats, and other details...By the way, they say both Marburg's and Ebola's reservoir is Egyptian Rousette bats.
So what is here defined as an "outbreak"? One person labelled positive by PCR....















"I'm listening to heavy metal". Good one, but I don't believe it.
The level of toxicities these subsistence-scratching people are exposed to is astounding in it's breakdown, after reading just these two papers you quote here re the Congo. And not only the miners (including children), but everyone else "downstream", literally.
Toxicity is very real, with even mainstream acknowledgement, but Rockefeller medicine never lets poisoning get in the way of a good virus story. Here's one story re arsenic sent to me by JAMA (I let them send me their free stuff): https://jamanetwork.com/journals/jama/fullarticle/2841553 .....study in Bangladesh, referencing well water .... "Question: Is reduced arsenic exposure associated with reduced chronic disease mortality?"
"Findings: In this 20-year prospective cohort study of 11 746 adults in Bangladesh, participants with greater reductions in urinary arsenic had significantly lower mortality from chronic diseases, including cancer and cardiovascular disease, compared with those with persistently high exposure."
And after reading about monoclonal antibodies and "elephant man", coupled to my own research, it's one again emphasized, as you put it, big medicine is "predicated on giving people little bits of poison until they either get better on their own despite the poison,... or die from the poison."
Thanks for the Ghana/marburg reference. It brings up another little point; use of language, specifically that used to sensationalize, propagandize, or cause fear. There are plenty of search results for the marburg/Ghana story, so I just went with Wiki:
"In July 2022, an outbreak of Marburg virus disease occurred in Ghana.[1] Two positive cases were reported by Ghana on 8 July. After confirmation by the World Health Organization, it is the first such outbreak in Ghana. Two men aged 26 and 51 years old were infected with the disease and both cases resulted in fatalities. An additional case was identified, bringing the total to three.[2]"
Just to summarize, we have here 3 claimed cases, and this is called an OUTBREAK. If there happens to be 3 claimed cases of "flu" here in the state of Oregon, are we suffering an outbreak?
So Wiki sums up: "The outbreak was confirmed by the World Health Organization on 17 July 2022, making it the first such outbreak in Ghana.[11] The outbreak follows another that occurred in Guinea the previous year.[12]"
So, moving on to the Guinea OUTBREAK, I'm told:
"The index case, a 46-year-old farmer from Temessadou M'Boké village in Guéckédou prefecture, got his first symptoms on July 25.[6] The patient died on August 2. On August 3, a Polymerase Chain Reaction (PCR) test was conducted, returning a positive result for the Marburg virus on August 5. The WHO was informed of the first case the next day. On August 9, the Institut Pasteur Dakar in Senegal provided reconfirmation that the result was positive for the Marburg virus.[6] Sequencing of an isolate from the Guinean patient showed that this outbreak was caused by the Angola-like Marburg virus.[6]
"Guinea health authorities conducted contact tracing and monitored 170 known high-risk contacts of the index case. No new cases were detected for twice the length of the incubation period of the virus, in this case 42 day, so the outbreak was declared over around six weeks after it started.[2][1]
"WHO's Africa director Matshidiso Moeti, among others, praised Guinea's rapid and effective response to the outbreak.[7]"
What fun. Here we have an "index case" of ONE (that's number 1), leading to, or should I say "being" an outbreak. An outbreak of 1....
https://en.wikipedia.org/wiki/2021_Guinea_Marburg_virus_disease_outbreak
More fun stuff is described, including WHO specialists showing up to trap bats, and other details...By the way, they say both Marburg's and Ebola's reservoir is Egyptian Rousette bats.
So what is here defined as an "outbreak"? One person labelled positive by PCR....